Ipsoprubart (ELA026): Redefining Patient Outcomes
Ipsoprubart (ELA026): Redefining Patient Outcomes
Ipsoprubart: Targeted Myeloid Cell and T Lymphocyte Depletor
Ipsoprubart, formerly ELA026, is a monoclonal antibody specifically designed to address severe inflammatory disorders with aberrant myeloid cell and T lymphocyte activity. It induces rapid, potent, and targeted depletion of the circulating myeloid cells and T lymphocytes that drive inflammation, without disrupting the CD47/SIRPα immune checkpoint function.

Treating sHLH, Offering Hope
There are no approved therapies for sHLH. Current off-label treatments for sHLH carry significant long-term toxicity and limited efficacy.3,4 Even with these treatments, sHLH has high mortality during the first few months.5 Malignancy-associated HLH (mHLH) is the deadliest amongst the subtypes of sHLH, with a mortality rate of approximately 50% at 2 months.6
~50% Fatality
Within 2 months for
Malignancy-Associated HLH
Ipsoprubart Targets the Principal Cells Responsible for Driving Pathogenesis in sHLH

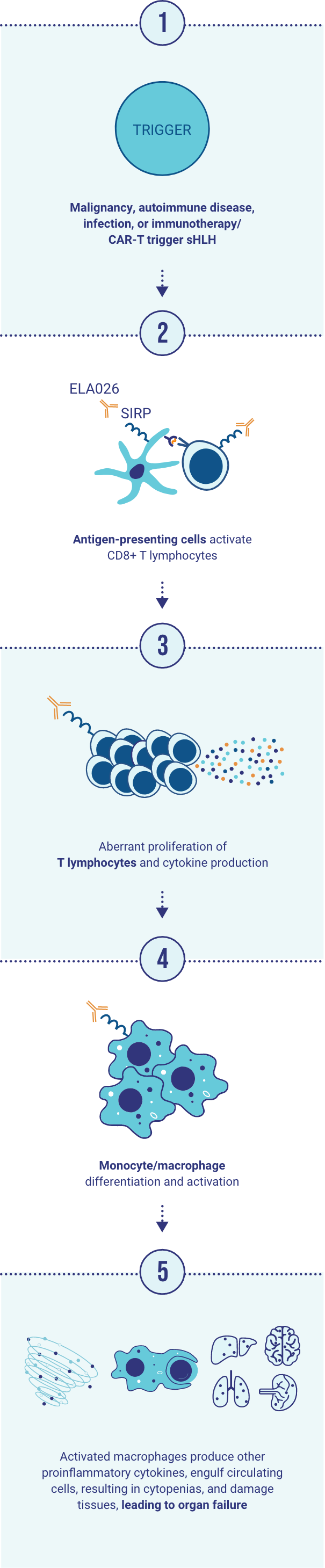
By targeting SIRP on the cell surface of myeloid cells and T lymphocytes, Ipsoprubart depletes the cells responsible for inducing the hyperinflammatory condition in sHLH.
By targeting SIRP on the cell surface of myeloid cells and T lymphocytes, Ipsoprubart depletes the cells responsible for inducing the hyperinflammatory condition in sHLH.
sHLH is a life-threatening disease in need of effective treatments.
Ipsoprubart has the potential to be a transformative treatment for patients with sHLH.
Ipsoprubart and ELA822 are investigational products currently under evaluation. FDA and other regulatory authorities have not approved ipsoprubart or ELA822 as safe or effective for any indication.
CAR-T=chimeric antigen receptor (CAR)-T cell.
References: 1. Otrock Z, Eby C. Clinical characteristics, prognostic factors, and outcomes of adult patients with hemophagocytic lymphohistiocytosis. Am J Hematol. 2015;90(3):220-224. doi:10.1002/ajh.23911 2. Trottestam H, Horne A, Aricò M, et al. Chemoimmunotherapy for hemophagocytic lymphohistiocytosis: long-term results of the HLH-94 treatment protocol. Blood. 2011;118(17):4577-4584. doi:10.1182/blood-2011-06-356261 3. Bergsten E, Horne A, Arico M, et al. Confirmed efficacy of etoposide and dexamethasone in HLH treatment: long-term results of the cooperative HLH-2004 study. Blood. 2017;130(25):2728-2738. doi:10.1182/blood-2017-06-788349 4. La Rosée P, Horne A, Hines M, et al. Recommendations for the management of hemophagocytic lymphohistiocytosis in adults. Blood. 2019;133(23):2465-2477. doi:10.1182/blood.2018894618 5. Abdelhay A, Mahmoud A, Mostafa M, et al. Delay in treatment of adult hemophagocytic lymphohistiocytosis is associated with worse in-hospital outcomes. Ann Hematol. 2023;102(11):2989-2996. doi:10.1007/s00277-023-05271-w 6. Lionel AC, Long JP, Prakash R, et al. Differing Inflammatory Profiles and Survival Outcomes of Cytokine Storm Arising from CAR T-Cell Therapy, Covid, and Malignancy-Associated HLH in Patients with Hematological Malignancies. Poster presented at the American Society of Hematology 2023. Poster: SUN-3507.